La maladie de Parkinson est la deuxième maladie neurodégénérative la plus courante, caractérisée par des tremblements, des mouvements ralentis, de la rigidité et des troubles cognitifs. La maladie de Parkinson affecte les neurones dopaminergiques de la substantia nigra du mésencéphale.
Une caractéristique particulière de la maladie de Parkinson est l'accumulation d'α-synucléine dans les neurones dans le cadre d'inclusions protéiques, les corps de Lewy. Comme les patients atteints d'autres maladies neurodégénératives, les patients atteints de la maladie de Parkinsons ont des biomarquers et des symptomes qu'on associe habituellement à d'autres maladies.
Il est à noter que 60% des malades d'Alzheimer ont des dépôts d'α-synucléine dans l'amygdale, et que certains patients atteints de maladie de Parkinson ont une accumulation d'Aβ dans le cerveau. Cela suggère que des voies spécifiques menant au développement de la maladie de Parkinson ou de la maladie d'Alzheimer convergent, provoquant l'apparition de signes communs.
Le rôle du cholestérol dans la maladie de Parkinson reste controversé. Un HDL sérique plus élevé est associé à une fonction cognitive plus faible chez les femmes atteintes de MP.
Une étude de radeaux lipidiques isolés du cortex frontal de sujets atteints de maladie de Parkinson à un stade précoce a montré une diminution des acides gras polyinsaturés sans modification du contenu en cholestérol et en sphingomyéline.
L'α-synucléine comprend deux domaines de liaison au cholestérol et le cholestérol membranaire affecte son agrégation. Théoriquement, la synucléine peut perturber l'intégrité du radeau lipidique, en interagissant avec le cholestérol.
La privation de nourriture (contrairement à ce qui est souvent répété) provoque l'agrégation de l'α-synucléine et l'apoptose, qui est associée au stress du réticulum endoplasmique, suivie d'une augmentation de la synthèse du cholestérol. Dans la maladie de Parkinson, la concentration de certains oxystérols augmente dans le cerveau en réponse à la surproduction d'espèces réactives de l'oxygène. Une alimentation riche en cholestérol réduit le rapport 24 OHC/27 OHC dans le cerveau et augmente le niveau d'α-synucléine dans la substantia nigra sans altérer le taux de cholestérol cérébral.
Plusieurs oxystérols sont associés à des maladies liées à l'âge telles que les maladies cardiovasculaires, les maladies oculaires (cataracte, dégénérescence maculaire liée à l'âge), certaines maladies neurodégénératives et les cancers. Les activités des oxystérols dans ces maladies pourraient être dues à leurs activités pro-oxydantes et pro-inflammatoires et à leur capacité à agir sur les organites cellulaires (mitochondries, peroxysomes, lysosomes) qui peuvent contribuer à activer l'apoptose et l'autophagie. Il existe des arguments soutenant que les oxystérols jouent un rôle important dans la progression de l'athérosclérose qui est impliquée dans plusieurs maladies cardiovasculaires.
Les scientifiques pensent depuis quelque temps déjà
que l'hyperlipidémie est associée à un risque accru de maladie de Parkinson. En effet, les niveaux de 27-hydroxycholestérol (27-OHC), un oxystérol, sont augmentés dans le cerveau et le liquide céphalo-rachidien des patients atteints de la maladie de Parkinson.
 Cependant, il reste difficile de savoir si cet oxystérol joue un rôle dans l'agrégation et la propagation de l'α-synucléine. L'objectif de scientifiques de Wuhan en Chine, était de déterminer si le 27-OHC régule l'agrégation et la propagation des α-synucléine.
Cependant, il reste difficile de savoir si cet oxystérol joue un rôle dans l'agrégation et la propagation de l'α-synucléine. L'objectif de scientifiques de Wuhan en Chine, était de déterminer si le 27-OHC régule l'agrégation et la propagation des α-synucléine.
Les auteurs ont étudié les deux aspects, administration et réduction de 27-OHC. Dans le premier cas, les scientifiques ont administré en sous-cutanée du 27-OHC à successivement de l'α-synucléine recombinante purifié, des cultures neuronales et un modèle murin (de souris de laboratoire) de la maladie de Parkinson. De plus, des souris knock-out CYP27A1 ont été utilisées pour étudier l'effet de la réduction du 27-OHC sur la pathologie α-synucléine in vivo.
Certes la physiologie de la souris n'a guère de point commun avec la physiologie humaine, mais c'est un progrès par rapport aux études in-vitro et celà pourrait encourager des études pré-cliniques utilisant des petits primates.
Leurs résultats confirment que 27-OHC accélère l'agrégation de α-synucléine et active l'activité d'ensemencement des fibrilles α-Syn. De plus, les fibrilles α-synucléine modifiées par 27-OHC se localisent dans les mitochondries et induisent un dysfonctionnement mitochondrial et une neurotoxicité.
L'injection de fibrilles α-synucléine modifiées par 27-OHC induit une propagation accrue de la pathologie α-synucléine et de la neurodégénérescence dopaminergique par rapport aux fibrilles α-synucléine pures. De même, l'administration sous-cutanée de 27-OHC facilite l'ensemencement de la pathologie α-Syn.
Au contraire, la suppression génétique du cytochrome P450 27A1, l'enzyme qui convertit le cholestérol en 27-OHC, améliore la propagation de l'α-synucléine pathologique, la dégénérescence de la voie dopaminergique nigrostriée et les déficiences motrices.
Ces résultats indiquent que le métabolite du cholestérol 27-OHC joue un rôle important dans la pathogenèse de la maladie de Parkinson. : 27-OHC favorise l'agrégation et la propagation de l'α-Syn. Les stratégies visant à inhiber l'axe CYP27A1-27-OHC pourraient être prometteuses en tant que traitement modificateur de la maladie pour stopper la progression de la pathologie α-synucléine dans la maladie de Parkinson. Le plus simple pour les patients est probablement d'adopter une alimentation pauvre en cholestérol et pour les scientifiques d'étudier les effets de administration de statine chez les malades de Parkinson.
Ces études ont déjà été abordés dans des publications récentes. Celle-ci aborde les effets du candesartan, simvastatin, and du fasudil chez des rats de laboratoire modèles de la maladie de Parkinson.
Celle-là fait une étude similaire de la simvastatin chez des rats.
Dans les deux cas les statines utilisées semblent avoir un effet bénéfique contre la maladie de Parkinson.

 Naphthoquinones are antiprotozoal drugs. Protozoa are small organisms, which exist as solitary cells or colonies of cells. They live in water or in moist soil or inside an organism (in the lung mucus, the intestine, the paunch of certain animals, etc.). They are known to be responsible for many diseases such as malaria and certain dysentery, such as amoebosis.
Naphthoquinones are antiprotozoal drugs. Protozoa are small organisms, which exist as solitary cells or colonies of cells. They live in water or in moist soil or inside an organism (in the lung mucus, the intestine, the paunch of certain animals, etc.). They are known to be responsible for many diseases such as malaria and certain dysentery, such as amoebosis.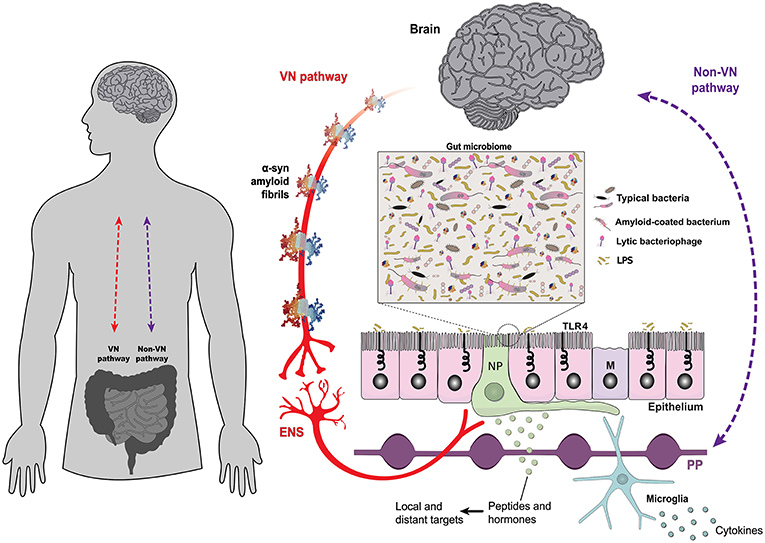 Certaines bactéries ont été particulièrement étudiées car en relation avec la maladie de Parkinson :
Certaines bactéries ont été particulièrement étudiées car en relation avec la maladie de Parkinson :
 This condition affects individuals, mostly adults over the age of 50, who physically act out their dreams during sleep, resulting in injuries to themselves or their bed partners. It's also suspected to be involved in premisses of Parkinson's disease. The study, published in the Journal of Neuroscience, presents a novel model that characterizes how REM sleep behavior disorder develops due to neurodegeneration associated with the accumulation of tau protein.
This condition affects individuals, mostly adults over the age of 50, who physically act out their dreams during sleep, resulting in injuries to themselves or their bed partners. It's also suspected to be involved in premisses of Parkinson's disease. The study, published in the Journal of Neuroscience, presents a novel model that characterizes how REM sleep behavior disorder develops due to neurodegeneration associated with the accumulation of tau protein.



 Deux théories concurrentes pourraient expliquer le dysfonctionnement visuel rétinien et d'ordre supérieur dans la maladie de Parkinson : un modèle suggère que des changements dégénératifs surviennent dans les régions corticales et se propagent à la rétine. l'autre propose au contraire que les cellules corticales et rétiniennes soient vulnérables à la dégénérescence dans la maladie de Parkinson.
Deux théories concurrentes pourraient expliquer le dysfonctionnement visuel rétinien et d'ordre supérieur dans la maladie de Parkinson : un modèle suggère que des changements dégénératifs surviennent dans les régions corticales et se propagent à la rétine. l'autre propose au contraire que les cellules corticales et rétiniennes soient vulnérables à la dégénérescence dans la maladie de Parkinson.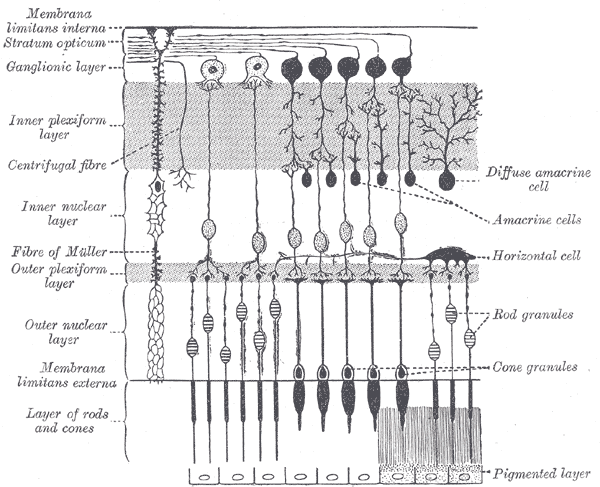 Source Wikipedia.
Source Wikipedia. Les scientifiques ont pour cela examiné de manière prospective la vision d'ordre supérieur (tolérance d'inclinaison et mouvement biologique) et l'épaisseur de la rétine (tomographie par cohérence optique dans le domaine spectral) chez 100 personnes atteintes de maladie de Parkinson et 29 témoins, avec des évaluations cognitives longitudinales au départ, 18 mois et 36 mois. Les scientifiques ont examiné si les mesures de base visuelles et rétiniennes prédisaient les scores cognitifs longitudinaux à l'aide de modèles linéaires à effets mixtes et si elles prédisaient l'apparition de la démence, la mort et la fragilité à l'aide de méthodes de temps jusqu'au résultat.
Les scientifiques ont pour cela examiné de manière prospective la vision d'ordre supérieur (tolérance d'inclinaison et mouvement biologique) et l'épaisseur de la rétine (tomographie par cohérence optique dans le domaine spectral) chez 100 personnes atteintes de maladie de Parkinson et 29 témoins, avec des évaluations cognitives longitudinales au départ, 18 mois et 36 mois. Les scientifiques ont examiné si les mesures de base visuelles et rétiniennes prédisaient les scores cognitifs longitudinaux à l'aide de modèles linéaires à effets mixtes et si elles prédisaient l'apparition de la démence, la mort et la fragilité à l'aide de méthodes de temps jusqu'au résultat. Nevertheless, the mechanistic basis for neuropathological and symptomatic heterogeneity remains unclear. Indeed differential neurotransmitter and receptor expression may underpin the selective vulnerability of several neuronal populations. So the lack of whole-brain spatial distribution maps of neurotransmitter receptors in patients with PD hampers research progress.
Nevertheless, the mechanistic basis for neuropathological and symptomatic heterogeneity remains unclear. Indeed differential neurotransmitter and receptor expression may underpin the selective vulnerability of several neuronal populations. So the lack of whole-brain spatial distribution maps of neurotransmitter receptors in patients with PD hampers research progress.