Here is a paper that outlines a new theory on the cause of Alzheimer's disease with implications for Parkinson's disease as well as ALS.
This is just speculation, based on almost only one fact: The expression of many genes is involved in this disease, so it would imply a global deregulation of the cellular machinery. Unfortunately, as usual in biology, this is a purely qualitative theory and, therefore, susceptible to many possibly contradictory interpretations. However, it is a theory that sees many neurodegenerative diseases as belonging to a spectrum rather than as distinct diseases. I endorse this point of view.
 Alzheimer's disease research has produced many hypotheses over the years, including cholinergic, inflammatory, viral, mitochondrial, tau, and amyloid. However, none of these hypotheses have led to treatments that can stop or reverse the disease. This leads to a search for new theories to explain these failures. But this may be because interventions occur too late in the disease progression, with brain damage irreparable and compensatory mechanisms saturated.
Alzheimer's disease research has produced many hypotheses over the years, including cholinergic, inflammatory, viral, mitochondrial, tau, and amyloid. However, none of these hypotheses have led to treatments that can stop or reverse the disease. This leads to a search for new theories to explain these failures. But this may be because interventions occur too late in the disease progression, with brain damage irreparable and compensatory mechanisms saturated.
Most publications ignore physiology, such as the importance of drainage in the cerebral lymphatic channels that have been discovered in recent years. This publication is no exception to this unfortunate trend, it is a discussion of the functioning of a cell in general, not even a brain cell like a neuron or an astrocyte, and the theory is even mostly not specific to humans or mammals, which still leaves one very skeptical. In this publication, the authors suggest that a disrupted nucleocytoplasmic transport system, linked to the formation of stress granules (SG), plays a central role. Cellular stress itself can have multiple causes independent of each other. There is no clear explanation why a general blockage of the cell would specifically lead to the appearance of beta-amyloid in Alzheimer's disease, nor that of alpha-synuclein in Parkinson's disease or TDP-43 in ALS.
In this model, cellular stress triggers SGs, which disrupt the movement of molecules between the nucleus and the cytoplasm, affecting RNA transport, chromatin accessibility, and alternative splicing. These changes lead to synaptic dysfunction, metabolic disorders, protein processing defects, and ultimately cell death. When this process propagates to brain regions, it results in clinical Alzheimer's disease.
The authors present a multistep mechanism linking SGs, NCT dysfunction, and amyloid propagation: * SG formation disrupts nucleocytoplasmic transport, altering gene expression and RNA localization. * Aβ clearance is decreased due to impaired lysosomal function, reduced proteostasis, and disrupted Aβ export. * Aβ production may increase via impaired APP processing. * Seeding and spreading of Aβ aggregates are facilitated by exosome dysregulation and chaperone sequestration. * Glial activation and BBB dysfunction further enhance Aβ diffusion in the brain.
The mention of ALS, FTD, and other conditions with similar transport disruptions strengthens the model's plausibility by showing how dysfunction of nucleocytoplasmic transport is implicated in multiple diseases.
Eukaryotic cells regulate the movement of molecules between the nucleus and the cytoplasm through nuclear pore complexes (NPCs), which are composed of nucleoporins. This transport is controlled by importins, exportins, and the protein Ran, which provides the energy for molecular movement.
Stress granules (SGs) are nonmembranous cytoplasmic structures that form in response to cellular stress, typically through phosphorylation of eukaryotic initiation factor 2 (eIF2α). During transient stress, SGs help cells recover, but during chronic stress, such as in Alzheimer's disease (AD), SGs abnormally persist and sequester key molecules, disrupting transcription and nucleocytoplasmic transport.
Disruption of nucleocytoplasmic transport in Alzheimer's disease (AD) was first reported in 2006, when cytoplasmic accumulation of nuclear transport factor 2 (NTF2) was observed in hippocampal neurons, even before the formation of neurofibrillary tangles (NFTs). This suggests that dysfunction of the transport system occurs early in the progression of AD. Analysis of gene expression data shows similar transport-related disruptions in tangle-bearing and non-tangle-bearing neurons.
Similar disruptions are observed in ALS, FTD, Huntington's disease, and even in non-neurological diseases such as cancer and heart failure. However, the specific transport disruptions vary by disease, likely due to different patterns of SG sequestration.
Some neurons maintain normal expression of the transport system and show enrichment in translational and neuronal function pathways, while others, with altered expression of the transport system, display stress-related pathways and deficits in mitochondrial function and metabolism. These findings are consistent with in vitro studies, suggesting that AD progresses along a continuum at the cellular level, ultimately leading to widespread neuronal dysfunction and clinical symptoms.
Conclusion The text suggests a causal role for SGs and transport dysfunction in AD, but much of the available supporting evidence comes from in vitro studies or studies of related diseases (e.g., ALS, FTD). The available direct in vivo evidence demonstrating SG-mediated pathology in AD patients is still limited.
Although the text discusses tau tangles and Aβ, their role appears secondary to SGs. Since amyloid and tau pathology remain at the core of AD research and therapeutic efforts, their relative downplaying constitutes a potential weakness.
The proposed model is primarily based on molecular and cellular studies, with little reference to clinical data.

 Curiously, scientists are rather looking to directly convert astrocytes into neurons, despite the enormous morphological difference between these two types of cells.
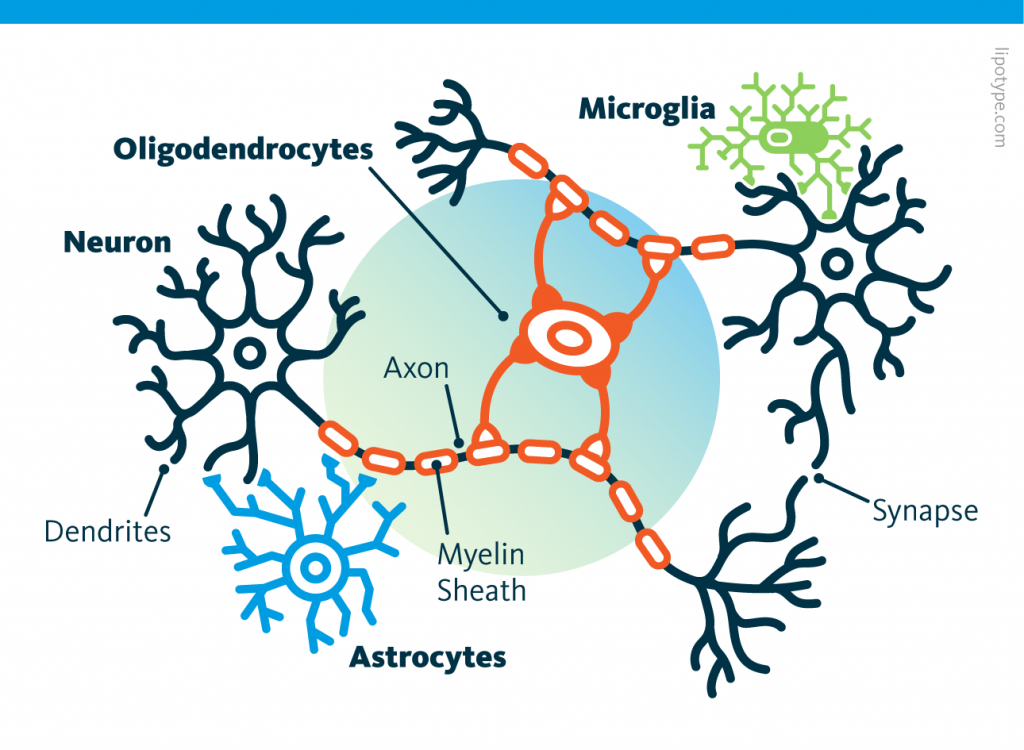
Curiously, scientists are rather looking to directly convert astrocytes into neurons, despite the enormous morphological difference between these two types of cells. Those other cells, which compose half of the brain's cells, are receiving more attention. There are multiple types but normally they are there to assist neurons in their task. A simplified view tells that neurons are a sort of plumbing system and the glial cells are the real actors in the brain.
Those other cells, which compose half of the brain's cells, are receiving more attention. There are multiple types but normally they are there to assist neurons in their task. A simplified view tells that neurons are a sort of plumbing system and the glial cells are the real actors in the brain. Source: Nephron via Wikipedia
Source: Nephron via Wikipedia
 Source: Peta
Source: Peta Running before learning aids in the formation of new memories, yet, running after learning promotes the forgetting of recently acquired information!
Running before learning aids in the formation of new memories, yet, running after learning promotes the forgetting of recently acquired information! Currently, the diagnosis of Alzheimer’s disease includes cognitive decline leading to dementia, associated with the observation of two major proteinopathies in the brain tissue. These two proteinopathies are plaques, formed by the aggregation of beta-amyloid proteins, and tangles, which are composed of hyperphosphorylated tau proteins.
Currently, the diagnosis of Alzheimer’s disease includes cognitive decline leading to dementia, associated with the observation of two major proteinopathies in the brain tissue. These two proteinopathies are plaques, formed by the aggregation of beta-amyloid proteins, and tangles, which are composed of hyperphosphorylated tau proteins. Ces cellules, contrairement aux neurones, ressemblent plus à leurs consoeurs du reste du corps à la fois par la morphologie et la durée de vie. A l'inverse un neurone est caractérisé par un ou plusieurs appendices dendritiques et axonaux et ne se reproduisent pas. Les neurones ont besoin des astrocytes et de nombreux autres types de cellules pour survivre.
Ces cellules, contrairement aux neurones, ressemblent plus à leurs consoeurs du reste du corps à la fois par la morphologie et la durée de vie. A l'inverse un neurone est caractérisé par un ou plusieurs appendices dendritiques et axonaux et ne se reproduisent pas. Les neurones ont besoin des astrocytes et de nombreux autres types de cellules pour survivre. Studies have shown that immune cells in the brain, particularly microglia, and astrocytes, are key regulators of the inflammatory response in the central nervous system and are involved in the pathogenesis of AD. These cells have various roles, including supporting neurons.
Studies have shown that immune cells in the brain, particularly microglia, and astrocytes, are key regulators of the inflammatory response in the central nervous system and are involved in the pathogenesis of AD. These cells have various roles, including supporting neurons.