This post is about a review of misdiagnosis in Amyotrophic Lateral Sclerosis (ALS). This refers to cases where individuals are incorrectly diagnosed with ALS when they actually have a different condition or disease.
ALS is a complex and challenging disease to diagnose accurately, as it shares some similarities with other neurological disorders. Misdiagnosis can lead to delays in appropriate treatment and management of the actual condition, resulting in potential harm to patients.
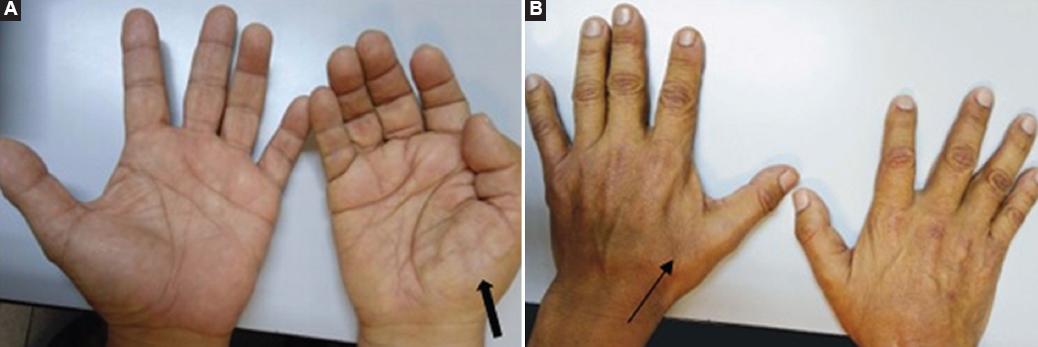 Hand surgeons are commonly the first providers to evaluate patients with undiagnosed ALS (the famous split-hand syndrome). So in early phases, the symptoms of amyotrophic lateral sclerosis (ALS) can mimic those of compressive neuropathies, such as carpal and cubital tunnel syndromes, especially early in a patient's clinical course. Scientists surveyed members of the American Society for Surgery of the Hand and found that 11% of active and retired members have performed nerve decompression surgeries on patients later diagnosed with ALS. Other scientists found that in 95% of cases, the diagnostic errors are, related to physician cognitive error that results from a lack of knowledge about the disease and inadequate decisions
Hand surgeons are commonly the first providers to evaluate patients with undiagnosed ALS (the famous split-hand syndrome). So in early phases, the symptoms of amyotrophic lateral sclerosis (ALS) can mimic those of compressive neuropathies, such as carpal and cubital tunnel syndromes, especially early in a patient's clinical course. Scientists surveyed members of the American Society for Surgery of the Hand and found that 11% of active and retired members have performed nerve decompression surgeries on patients later diagnosed with ALS. Other scientists found that in 95% of cases, the diagnostic errors are, related to physician cognitive error that results from a lack of knowledge about the disease and inadequate decisions
Several factors contribute to the potential for misdiagnosis in ALS:
Overlapping symptoms: ALS symptoms, such as muscle weakness, muscle atrophy, fasciculations (muscle twitches), and difficulty speaking or swallowing, can resemble symptoms of other neuromuscular or neurodegenerative disorders. Conditions such as spinal muscular atrophy, primary lateral sclerosis, Kennedy's disease, multifocal motor neuropathy, and certain forms of muscular dystrophy may exhibit similar symptoms, leading to confusion in diagnosis.
Variability in symptom progression: ALS symptoms can vary in their presentation and progression among individuals. Some patients may experience rapid progression, while others have a slower disease course. This variability can make it challenging to differentiate ALS from other conditions that may share similar symptom patterns.
The diagnosis of ALS is primarily based on clinical examination, medical history, and the exclusion of other potential causes. There is no single definitive test for ALS, making the diagnosis subjective and reliant on the judgment and experience of healthcare professionals. This subjectivity can increase the risk of misdiagnosis.
Limited accessibility to specialized testing: Certain diagnostic tests, such as electromyography (EMG) and nerve conduction studies, can help in confirming ALS by evaluating the electrical activity of muscles and nerves. However, these tests may not be readily available in all healthcare settings, leading to potential delays or errors in diagnosis.
Disease heterogeneity: ALS is a heterogeneous disease, meaning it can manifest differently in different individuals. Some cases may present with atypical features or unusual disease progression, making it more challenging to reach an accurate diagnosis.
To minimize the risk of misdiagnosis in ALS, it is crucial to follow a comprehensive diagnostic approach that includes thorough clinical evaluations, specialized testing (such as EMG), and consultation with neurologists or neuromuscular specialists experienced in diagnosing and managing ALS. Additionally, regular follow-up assessments and monitoring of symptoms are important to ensure accurate diagnosis and appropriate management throughout the disease course.
It is important to be aware of the history, signs, and symptoms of ALS to provide an accurate diagnosis and prevent unnecessary morbidities, such as nerve decompression surgery, which invariably results in poor outcomes. The major "red flag" symptoms warranting further work-up include weakness without sensory symptoms, profound weakness and atrophy in multiple nerve distributions, progressively bilateral and global symptoms, presence of bulbar symptoms (such as tongue fasciculations and speech/swallowing difficulties), and if surgery is performed, failure to improve. If any of these red flags are present, we recommend neurodiagnostic testing and prompt referral to a neurologist for further work-up and treatment.
It is worth noting that misdiagnosis can also occur in the opposite direction, where individuals with other conditions are mistakenly diagnosed with ALS. Therefore, seeking multiple medical opinions and consulting with specialists can help reduce the likelihood of misdiagnosis and ensure the most accurate diagnosis and appropriate care.